


Regarding the HFCS Structural Change and Increase in Human Depression in the US
An ‘environmental assessment’
Introduction
Before the invention of modern carbon monoxide detectors (or forced air mine ventilation), miners used caged canaries to test for the accumulation of dangerous amounts of carbon monoxide in coal mines. Being more sensitive than the miners to CO, if a canary ceased singing and fell from its perch, then the miners knew it was time for them and the canaries to exit the mine.
Speaking of warning signs from the sensitive, here’s a rather ominous graph showing a significant increase in incidence of the physical symptoms of depression in US 12th graders. The greater the Y-axis value, the greater the incidence and/or severity of the graph-denoted difficulties associated with mental depression:

It is critically important to note, however, that post-pubescent girls and women make up the bulk of the depressed subpopulation of the US, with the girls and younger women (14-25 y.o.) evidencing double or more the male incidence of depression. This being the case, the increases in somatic symptoms of depression in females shown in the graph above have been dampened by dilution with the lower depression symptom scores of less depressed 12th grade males. The actual magnitude of the increase in occurrence of female depression in the US (and elsewhere) – and its contrast with that of males -- is more accurately denoted below, using the sexually bifurcated American teenaged population as sample:

The next graph shows the same sex-linked relationship of depression in older American age groups:

The Two Tryptophan Metabolic Pathways and the Symptoms of Depression
Dietary tryptophan moves through two separate metabolic pathways -- provided it is successfully absorbed in the small intestine -- producing serotonin, melatonin, and niacin as illustrated below.

Serotonin is believed to play a role in disorders related to mood, anxiety, psychosis, and pain, and affects cognition, learning, and memory. Melatonin is, among other things, a notable regulator of sleep-wake timing and duration. Niacin prevents pellagra, a vitamin deficiency physically marked by skin and mouth lesions, anemia, headaches, and tiredness, and by psychosensory disturbances (pain, sensitivity to bright lights, odor intolerance, and dizziness), psychomotor disturbances (restlessness, tenseness, and a desire to quarrel), as well as generalized emotional disturbances.
Note in the following list that the catchall symptoms of depression significantly overlap with symptoms that can result from deficiencies in precursor tryptophan and/or the unbalanced production of the metabolic products serotonin, melatonin, and niacin. The tryptophan-dependent deficiencies strongly suspected to be associated with each depression symptom are placed in [brackets]. Note here that selective serotonin reuptake inhibitors (SSRIs) are the most widely prescribed antidepressants in the United States. The pot-pourri of the major signs and symptoms of a person suffering from depression include:
• Feelings of sadness, emptiness, or hopelessness [serotonin]
• Irritability, angry outbursts, or low frustration tolerance [serotonin, niacin]
• Loss of interest in or ability to enjoy usual activities, from sex to sports [serotonin, niacin]
• Sleep disturbance, whether inability to sleep or sleeping too much [melatonin, niacin]
• Fatigue and lack of energy; everything feels effortful [niacin, melatonin]
• Appetite disturbance, including loss of interest in eating and weight loss or overeating and weight gain [serotonin]
• Anxiety, agitation, and restlessness [niacin]
• Slowed thinking, moving, or talking [niacin, serotonin]
• Feelings of worthlessness and guilt, a focus on past failure, self-blame [serotonin]
• Difficulty concentrating, remembering things, and making decisions [serotonin, niacin]
• Recurring thoughts of death [serotonin]
• Physical pain such as headaches or back pain that has no clear cause [serotonin, niacin]
The Two Clumsy Elephants Banging around in Tryptophan’s China Shop: Estrogen and Added Dietary Fructose
A group of researchers (D. Fuchs, principal investigator) at the Institute for Medical Chemistry and Biochemistry, the University of Innsbruck, Austria, carried out a series of studies into the biochemical and neurological effects of tryptophan that support a simple physical, rather than a complex cultural or socio-political, explanation for the increase in incidence of depression in post-pubescent females since (at least) the 1980s. The Austrians’ work, among other things, indicates that in post-pubescent females, but not in males, the disorder of intestinal fructose malabsorption causes insufficient absorption of tryptophan by the intestine, consequently reduced levels of tryptophan in the blood, serotonin and melatonin in the brain, and niacin in the cells – all of which can lead to mental depression and its various mood and behavioral disturbances.
The Austrians believe that unabsorbed free fructose bonds with dietary proteins including the amino acid tryptophan in a Maillard reaction. This abnormal sugar-protein bonding within the digestive system makes intestinal absorption of tryptophan in food much less efficient, thus creating a dietary tryptophan deficiency even when tryptophan dietary intake is otherwise sufficient.
Ledochowski, Sperner-Unterweger, Widner, and Fuchs, 1998, summarize their findings:
“Having made the observation that persons with fructose malabsorption very often seem to present not only with signs of irritable bowel syndrome but also with signs of pre-menstrual syndrome and mental depression, it was of interest to establish whether such an association could be demonstrated in patients.
Subjects with fructose malabsorption showed a significantly higher score in the Beck’s depression inventory than normal fructose absorbers. This was true especially for females.”
Shibata and Toda (1993, 1997) further showed that estrogens strongly interfere in the later conversion of digestively-absorbed tryptophan to niacin, making post-pubescent/pre-menopausal women also much more susceptible to niacin deficiency and pellagra during pregnancy and during specific parts of their menstrual cycle:1
“In our data, the tryptophan to nicotinamide2 conversion was decreased to about one-third of that of the control group (Fig. 2). This demonstrates that the increases in progesterone and estrone in body tissues at such times as pregnancy and the postovulatory phase induce the decrease in the conversion of tryptophan to nicotinamide: It also suggests that the twofold [increased] incidence of pellagra deaths in women is attributable to the female hormones.”
All in all, Shibata and Toda’s (1993, 1997) and Ledochowski et al.’s (1998) observations mean that post-pubescent/pre-menopausal females who malabsorb fructose are also the most apt to evidence physical, mental, and behavioral depression symptoms. These symptoms appear to be generated by the combined effects of the industrial introduction of much additional free fructose to the human diet of the Westernized nations, and by the natural fluctuations in estrogens created by the ordinary female hormone cycle and its temporary alternative, pregnancy. The net effect of these factors is to induce significant dietary tryptophan deficiencies in many post-pubescent/pre-menopausal females, crippling the normal operation of their tryptophan metabolism and thus causing the various symptoms of depression.
Unfortunately, tryptophan is the least abundant amino acid in foods, and, because humans are unable to produce their own supply of this amino acid, tryptophan is an essential component of the human diet. The following two tables show that— the further exacerbating effects of fructose and estrogen aside — tryptophan deficiency is, even under the best of times and circumstances, an easy state for any human to enter.


The Manageable Fructose Elephant and the US Depression Data
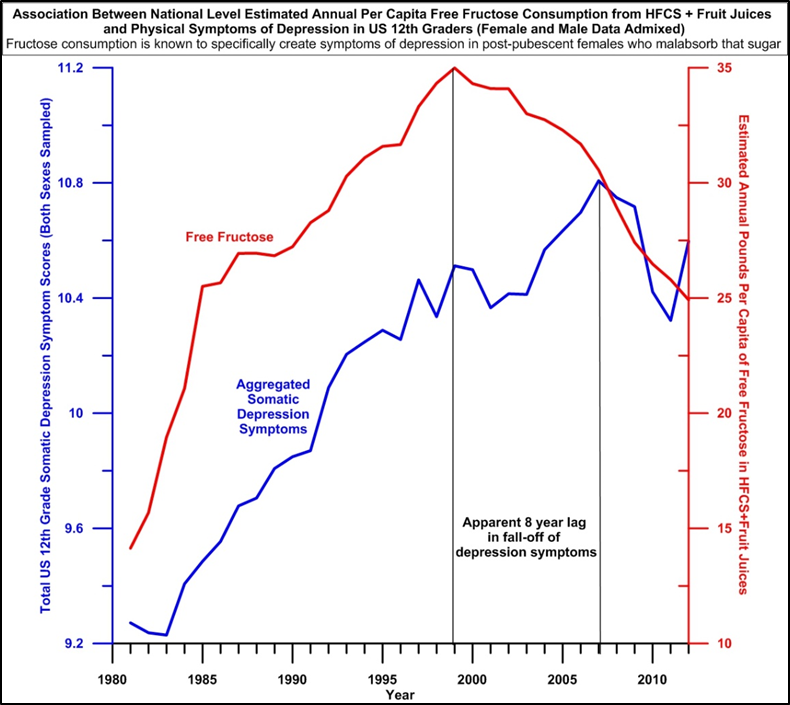
In the next graph, the aggregated (total score) female-dominated depression symptom data for US 12th graders (for data source, see again the first graph of this post) reveals a strong relationship between the increase in the amount of free fructose in the American diet and the increase in depression symptoms over the same time period. Examining this graph, note that high fructose corn syrup was first introduced to the US in the late 1960s/early 1970s and that consumption per capita of this new sweetener within the US grew most rapidly in the early 1980s – during the same period of time that saw the greatest increase in the symptoms of depression in American female 12th graders.
Fortunately, the negative effects of excessive dietary fructose are easily managed and reversable. See Choi et al., 1998, and Ledochowski et al., 2000. Ledochowski et al., in particular show that both physical and mental problems caused by fructose in fructose malabsorbers are rapidly improved by changing diet to avoid fructose. After a period of only four weeks of dietary fructose restriction, depression scores were reduced by about 65% and fructose abstainers also experienced significant reductions in their previously chronic gastrointestinal problems.
Fructose and the Human Gut, Normally
As previously remarked, it turns out that excess amounts of fructose can not only cause and maintain obesity -- and many other metabolic problems -- over the long run, but ingestion of this simple sugar can also create acute problems in the short run because of the phenomenon of fructose malabsorption. Acute gastrointestinal difficulties like abdominal pain and cramps, bloating, and diarrhea are frequently caused by fructose malabsorption. These problems come about because fructose that is normally absorbed in the small intestine instead passes on down to the large intestine where bacteria break down the sugar, producing gas and other fermentation products, and where increased osmotic load can often draw body water back out into the lower intestine, causing diarrhea and loose stools.3
The fructose “malabsorption” of Ledochowski et al., 1998, and others is relative, however, in that all humans have a limited but yet individually varying biological capacity to absorb a large, concentrated oral liquid fructose feeding (a bolus) in their small intestines. Young children, for example, have an extremely low capacity to absorb liquid dietary fructose that only very gradually increases with age. See below.


Most adults, on the other hand, can ingest up to 50 grams of free fructose (as in a HFCS-sweetened soft drink or a natural fruit juice) all at one time. Current (2020) average adult daily intake of fructose in the US and other Western countries is, in fact, about 50 grams, an observation indicating that the average Western adult exists perpetually on the edge of being a fructose malabsorber and suffering the physical and mental consequences of this unhappy state.
For reference, see the following graph showing the free fructose contents of a liter of the various high fructose corn syrup-sweetened soft drinks sold in the US, and note that about the same amount of fructose is also found in a liter of most natural fruit juices.4

Summary and Speculations
Clinic and epidemiological data indicate that the structural change in Western diet caused by the late 1960s/early 1970s introduction of high fructose corn syrup has also created a very strong structural change in the mental and physical health of the humans ingesting the substance. Post-pubescent/pre-menopausal women with relatively low capacity to absorb fructose in their small intestines are especially sensitive to the deleterious metabolic effects of increased fructose in their diets, and have exhibited increased symptoms of mental depression as a result of this sugar’s increased presence in the modern industrial diet. These women, with their especially sensitive tryptophan pathways, could, figuratively speaking, be considered to be ‘canaries within a fructose factory’.

Because an adult eating a Western diet now consumes, on average, 50 grams of fructose each day, and because this amount of fructose marks the tipping point into a harmful state of fructose malabsorption and tryptophan deficiency, it is suspected that subclinical cases of both depression and pellagra are now quite prevalent in Western populations. It is further suspected that the socio-political polarization and conflict, as well as governmental/administrative, scientific, and healthcare dysfunction, currently being exhibited in Westernized societies are not the result of some kind of political or cultural or idealogical ‘wrongthink’, but are instead the thoroughly penetrating manifestations of one root cause of poor nutritional health and its mental effects.
As a review relevant to the last paragraph, here are the mental and behavioral symptoms associated with disturbances of the two tryptophan pathways signaled by depression and/or pellagra. Note the considerable symptom overlap between depression and pellagra.
Depression:
Feelings of sadness, emptiness, or hopelessness
Irritability, angry outbursts, or low frustration tolerance
Loss of interest in or ability to enjoy usual activities, from sex to sports
Sleep disturbance, whether inability to sleep or sleeping too much
Fatigue and lack of energy; everything feels effortful
Appetite disturbance, including loss of interest in eating and weight loss or overeating and weight gain
Anxiety, agitation, and restlessness
Slowed thinking, moving, or talking
Feelings of worthlessness and guilt, a focus on past failure, self-blame
Difficulty concentrating, remembering things, and making decisions
Recurring thoughts of death
Physical pain such as headaches or back pain that has no clear cause
Pellagra:
Trouble sleeping
Weakness
Mental confusion or aggression
Restlessness, tenseness and a desire to quarrel, increased preparedness for motor action
Emotional disturbances
Nicotinamide is the slightly altered amide form of niacin. Both chemical forms – niacin and nicotinamide -- have the same vitamin behavior.