


What’s Known about Quercetin or Rutin Dosing and the Resulting Quercetin Values in Human Intercellular Fluid (Plasma)
Caution indicated
This very last springtime 2023 blurb on Grundvilk might be of interest to people contemplating trying to experimentally improve their health through intentional (rather than fortuitous) consumption of quercetin- and/or rutin-containing foods, or by the direct ingestion of quercetin or rutin supplements. For more background on the whole subject, see this previous post -- and this one, too.
Currently published clinical data indicate that even a very small amount of orally-consumed quercetin will reduce a measurable fraction of the senescent cell burden in humans. From just a little greater than nil µmoles/liter up to 10 µmoles/liter, senescent human umbilical vein endothelial cells (“HUVEC”), susceptible to quercetin, die off without much harm to normal, non-senescent cells. At higher than 10 µmoles/liter quercetin concentrations, however, quercetin increasingly interferes with the growth and proliferation of normal endothelial cells. See the graph below for depiction of the above-described cell states.

In slight contrast to these laboratory observations of very young endothelial cells, test of quercetin’s effect on adult human arterial vascular endothelial cells indicates that quercetin begins to kill senescent adult endothelial cells only at about the quercetin concentration of 4 µmoles/liter, and begins significantly harming non-senescent proliferating cells at quercetin concentrations of greater than 8 µmoles/liter.1
These being the observed in vitro laboratory cases with human cells, it would be helpful to have some idea what in vivo oral quercetin and/or rutin doses could result in helpful or potentially harmful levels of quercetin in human intercellular fluid/plasma. Fortunately, a small clinical study has been carried out with healthy human subjects (n=16) that determined plasma quercetin levels under different oral dosing regimes. The study separately utilized quercetin itself and rutin as quercetin sources. The two summary profiles provided below illustrate the averaged results for each of the two source compounds.
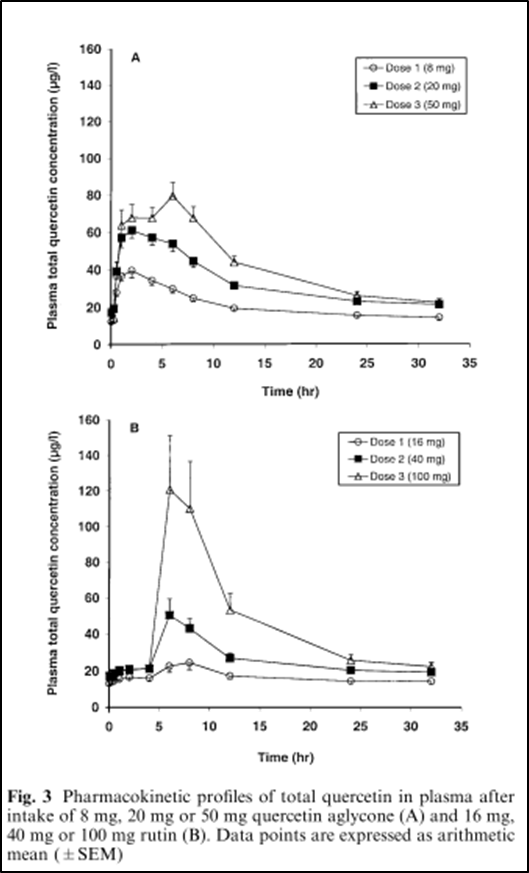
Clearly, there is a positive relationship between the size of the dose taken and the level of plasma quercetin resulting. Note that in both the oral quercetin and oral rutin dosing cases, peak plasma quercetin levels last for at least two hours under all oral dosing levels of the senolytics. This duration of maximal quercetin concentration is very important because, as Mayo Clinic’s James Kirkland states:
“Senolytics start working very quickly – it only takes a couple of hours of exposure to senolytics to start killing senescent cells.”
The following two graphs were generated from re-graphing of only the peak quercetin concentrations in µg/l for each dose and each compound shown in the two different pharmacokinetic profiles of the Figure above.


Evidently there are concrete biochemical reasons why rutin ingestion results in much higher plasma quercetin concentrations than is possible through oral consumption of quercetin. ChatGP conveniently (and very circumspectly) sums up the relevant research to date:
“Some research suggests that rutin may be hydrolyzed to quercetin in the lower gut, specifically in the colon, by gut microbiota or other enzymes, and that this quercetin may then be absorbed into the body through the lymphatic system, bypassing the liver's first-pass metabolism.
Quercetin is known to undergo extensive metabolism in the liver, where it is subjected to processes such as glucuronidation, sulfation, and methylation, which can reduce its bioavailability and affect its pharmacokinetics. However, when rutin is hydrolyzed to quercetin in the colon, it may be absorbed into the lymphatic system through specialized lymphatic vessels called lacteals, which are located in the gut lining and are responsible for absorbing dietary fats and fat-soluble substances.
This potential route of absorption through the lymphatic system may allow quercetin to bypass the liver's first-pass metabolism, which could result in higher systemic levels of quercetin compared to quercetin ingestion alone. This could potentially enhance the bioavailability and bioactivity of quercetin, as it may be less extensively metabolized in the liver and more readily available for systemic distribution.”
So, the dosing data provided here indicate that both quercetin and rutin supplementation raise blood plasma quercetin levels up to the point where some of the health-hindering burden of senescent cells will be removed. Because of the apparent influence of the liver, however, quercetin ingestion results only in plasma quercetin concentrations that fall onto the far left hand side of the x-axis of first graph of this post, resulting in a relatively small amount of senescent cell reduction. Rutin consumption on the order involved in the historical Hunza/Burusho springtime diet, on the other hand, apparently achieves plasma quercetin concentrations that are quite close to the optimal 10 µmole/l level necessary for maximally reducing senescent cell burden while minimizing damage to normal cells.
Mayo Clinic’s James Kirkland has this to say about how often senolytic compounds appear to need to be consumed on an ongoing basis in order to significantly reduce senolytic cell burden:
“Since new senescent cells take 10 days to 6 weeks to form, these senolytic agents can be administered in a hit and run manner – once or twice if there is an insult like radiation that’s not repeated, and do that periodically as new cells form. In those experimental situations the [senolytic] drugs can be given once every two weeks or once in a month and that has the same effects as giving these agents continuously. We are not trying to occupy a receptor or inhibit an enzyme, not looking for a steady state of the compound in blood, we’re trying to get rid of a cell type, allow these cells to kill themselves. Two to three hours of exposure is enough to do so. And then it takes ~18 hours for the cells to kill themselves. So that’s why the hit and run manner works sufficiently.”
In conclusion, it will not hurt to replicate here a typical cautionary statement found at the end of all of the technical papers on senolytics and reducing senescent cell burden produced by the Mayo Clinic’s James Kirkland research group. At least partially in the interest of caution, the Mayo Clinic writers always state something like this in their final statements:
“Consistent with the Unitary Theory, senolytics appear to restore progenitor dysfunction, attenuate tissue inflammation and alleviate age- and disease-related metabolic dysfunction across cell types and tissues. Senolytics appear to delay, prevent or alleviate multiple age-related conditions and chronic diseases and enhance healthspan and lifespan in experimental animals. Therefore, these agents could lead to interventions for humans that delay, prevent or treat senescence- and age-related conditions – if clinical trials continue to demonstrate effectiveness and low toxicity. However, unless and until such clinical trials are completed and demonstrate safety, tolerability, target engagement and effectiveness, candidate senolytics should not be prescribed or used by general patient populations. They should only be administered in the course of carefully monitored clinical trials.”
Given that quercetin per se is omnipresent in traditional human plant foods and its peak plasma concentration is strongly limited by the governing action of the liver, comparatively less caution likely needs to be exerted with regard to its use as a dietary supplement.
On the other hand, because rutin bypasses the liver, its possible use as a senolytic supplement should be considered and handled very carefully, less peak plasma quercetin concentrations get high enough to substantially harm growth and operation of normal (non-senescent) cells. It seems entirely possible that part of the reason the Hunza/Burusho viewed rutin-rich bitter (tartary) buckwheat as a “frankly detested” part of their traditional annual diet was because of quercetin-derived side effects sometimes encountered during the limited time of the year these people were forced to subsist on these rutin-rich seeds.
These possible side effects of rutin consumption include:
· blurred vision
· dizziness
· dull ache or feeling of pressure or heaviness in legs
· fluid accumulation in the knee
· headache
· itching skin near damaged veins
· nervousness
· pounding in the ears
· red, scaly, or itchy skin
· slow or fast heartbeat
· swollen feet and ankles
Some anecdotal reports from people who have taken rutin also say it may cause constipation.
The results of the studies on the two different endothelial cell types are very similar, despite the representations of the authors of the more recent research report on adult endothelial cells to the contrary. If in doubt about this, examine the graphs of the linked second study and judge for yourself.