


Zinc and Its Ionophores
Second in a series concerning non-pharmaceutical work-arounds to human immunosenescence and COVID19
Reprise and Introduction
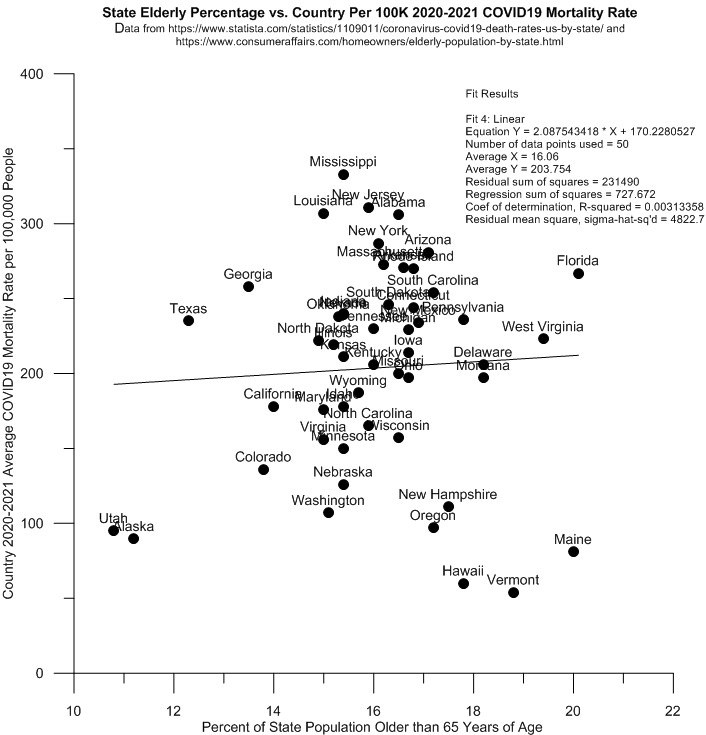
Recall that mortality data show that increasing age per se is not at all a reliably predictive determinant of the likely individual outcome of a COVID19 infection. This is because the senescence-related biological weaknesses that eventually come with age do not develop at the same rate and at the same age in all people -- and at all places.
A plot of the state level percent of elderly in population vs. 2020-2021 COVID19 death rates per 100,000 people for each US state supports this assertion. See the graph below. While states like Louisiana and Mississippi with a relatively small proportion of elderly people in their populations suffered quite high death rates (>300 deaths/100,000 people) due to COVID19 over 2020-2021, other states like Maine and Vermont with much higher than average percentages of older people within their borders experienced some of the very lowest COVID19 death rates in the nation (<100 deaths/100,000 people). Health-wise speaking, then, getting older in a state like Vermont or Maine is not at all as generally dire as the process of growing old in Louisiana or Mississippi.
Recall also that at the individual scale, various researchers and clinicians have provided credible evidence that supplementation with the following agents can help prevent and/or ameliorate the worst effects of a COVID19 or other respiratory virus or bacterial infections:
1. Zinc
2. Various zinc ionophores
3. Vitamin D
4. Arginine and citrulline (both are nitric oxide precursors)
5. N-Acetyl Cysteine (“NAC” is a glutathione precursor)
6. NAD+ precursors like niacin
This post will briefly review the scientifically-demonstrated biochemical actions of zinc and its ionophores (once again, zinc ionophores are chemical complexing agents that are necessary for bringing blood-carried zinc into each human cell). The post will also provide some zinc- and zinc ionophore-related geographically-controlled evidence that appears to partially and reasonably explain why some state populations have experienced greater overall COVID19 mortality than other states.
Zinc and Its Ionophores: the History
Supplementation with zinc and/or the organic compounds, ionophores, that help this trace metal pass through cell walls into the cell interior, has been shown to be critical to the support and maintenance of human innate and adaptive immunity for more than 50 years, well before the apparent emergence of COVID19 in 2019.
According to Yasuda and Tsutsui (2016):
“The importance of zinc for human health has been recognized since the early 1960s. Zinc is an essential micronutrient required for the activity of more than 300 enzymes and 1,000 transcription factors and for the control of genetic expression. It also plays important roles in nucleic acid/protein synthesis, cell replication, and tissue growth and repair. Zinc deficiency is known to be associated with various pathological conditions, including impaired immunity, delayed wound healing, retarded growth, neural development disorders and degenerative diseases.”
Using a large sample of the Japanese population (n=28,424 people) , the same authors determined that by age 80, almost 20% of that nation’s people showed a pronounced zinc deficiency. Very significantly, moreover, only about 3% of the sampled population that was able to live on to reach the age of 90 was found to be zinc deficient.
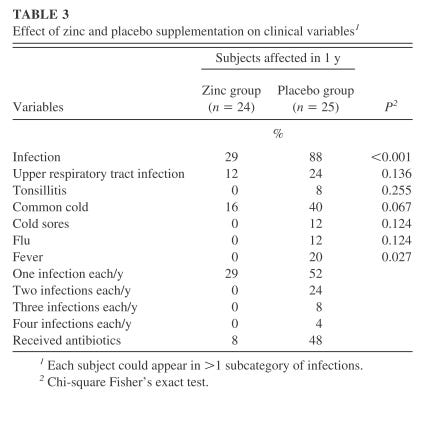
The central and critical roles that zinc plays in maintaining innate and adaptive immunity are related in detail by Shankar and Prasad (1998). A subsequent (2007) one year clinical study showed that 45mg/day oral zinc supplementation quite markedly reduced all classes of infection in most of the tested elderly (56-83 years old) compared to placebo group, thus successfully reactivating many previously moribund, senescing immune systems. Below see the ‘Table 3’ taken from that 2007 paper.
A detailed review of the multiple and generalized anti-viral roles that zinc plays can be found here. More specifically, the 2010 paper, entitled, “Zn2+ inhibits coronavirus and arterivirus RNA polymerase activity in vitro and zinc ionophores block the replication of these viruses in cell culture”, first clearly showed that cellular infection by coronaviruses is preventable by two separate zinc-dependent mechanisms, mechanisms dependent on the simultaneous presence of zinc ionophores like prescription HCQ (hydroxychloroquine), chloroquine, and [probably] ivermectin, or like polyphenol-containing plant compounds such as quinine, quercetin, or epigallocatechin-gallate.
The 2010 zinc and zinc ionophore paper (ibid.) clearly showed that, while ionophores or zinc alone can hinder coronavirus replication, synergistic combination of the two is much more effective at much lower concentrations of zinc:
“The reporter gene expression of both SARS-CoV-GFP and EAV-GFP was already significantly inhibited in a dose-dependent manner by the addition of PT [a zinc ionophore] alone. This effect was significantly enhanced when 2 mM [micromolar] of Zn2+ was added to the medium. We found that addition of ZnOAc2 alone also reduced virus replication, but only at levels that were close to the 50% cytotoxicity concentration (CC50) of ZnOAc2 in Vero-E6 cells (~70 mM [millimolar], data not shown). This is likely due to the poor solubility of Zn2+ in phosphate-containing medium and the inefficient uptake of Zn2+ by cells in the absence of zinc-ionophores. The combination of 2 mM PT and 2 mM ZnOAc2 resulted in a 98±1% and 85±3% reduction of the GFP signal for EAV-GFP and SARS-CoV-GFP, respectively. No cytotoxicity was observed for this combination of PT and ZnOAc2 concentrations.”
Note that at least as far back as 2004 it was also reported that orally administered zinc ionophores given by themselves can effectively inhibit the replicative activity of SARS viruses:
“Chloroquine is given prophylactically at a dose of 300 mg/week to people travelling to malaria endemic areas. If SARS re-emerges, chloroquine can be of great importance as prophylactic medication for people living in and travelling to the affected area. Chloroquine is ubiquitously available, of low cost, and easy to administer. It may be considered for immediate use in the prevention and treatment of SARS-CoV infections.”
It is evident, then, that Zelenko did not independently or arbitarily ‘invent’ his HCQ and zinc COVID19 preventive and prophylactic clinical therapy out of whole cloth, but instead “followed the science” and, like any competent applied scientist, resorted to a reading of the long-published medical research literature to initially locate a likely practical, effective, and safe treatment approach for his COVID19 patients.
Crawford’s tally of HCQ + zinc clinical study results from about a year ago follows. Note the similarity in effect achieved by this COVID19 therapeutic and preventive approach and that of the older, more generalized 2007 ‘Table 3’ viral and bacterial infection-reducing effects of zinc found earlier in this post.

Regional Environmental and Dietary Habits as Apparent Controls of the State to State Variation in Levels of COVID19 Mortality in the USA
The primary clinical approach to non-vaccine-related management of COVID19 has been to first identify agents, medicinal or dietary, that will buttress natural innate and adaptive immunity, and also dampen down and control the dangerous inflammation reactions created in various tissues and organs by the COVID19 virus. The second step in this approach is to preventively and prophylactically supplement patients with these identified agents to shore up threatened human immune systems against opportunistic COVID19 infection.
The conscious aims of human medical systems and medical practitioners aside, however, physical variations in the environment and geographic differences in diet inadvertently expose geographically-distributed human populations to significant variations in background levels of zinc, zinc ionophores, vitamin D, nitric oxide and its precursors, glutathione and its precursors, and NAD+ and its precursors.
Using statistical proxies for geographically different background environmental and dietary levels of these six agents, it has proven possible to predict a bit more than 80% of the state-to-state native variation in US COVID19 mortality rate. The statistically-estimated mathematical model of this environmental and biological system of COVID19 mortality-determining controlling factors will be described in the final post of this Substack series on human senescence work-arounds. Here, however, only simple scatter plots and their lines-of-best-fit will be used to show the geographic variation in background levels of zinc and its ionophores created by geographically-controlled geology and diet –- and the apparent effect of the geographic variation in levels of these agents on state-wide COVID19 mortality.
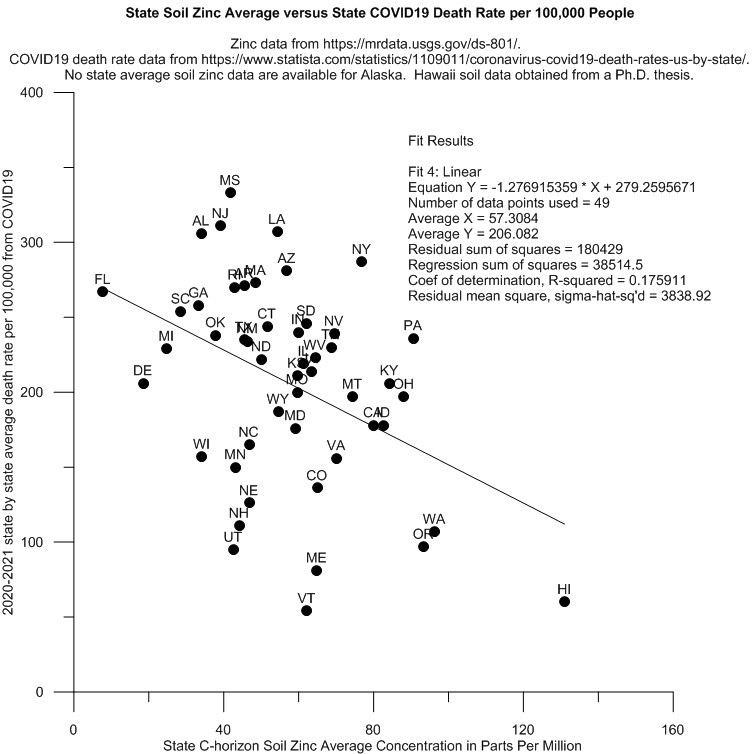
Not surprisingly, background (i.e., unsupplemented) human cellular zinc levels are ordinarily determined by the concentration of zinc in outdoor and indoor dust. The zinc in these dusts is absorbed chiefly by the human digestive system and the lungs. In turn, the concentration of zinc in indoor and outdoor dust is chiefly determined by 1) the chemical nature of the soil parent material (i.e., the rock or other materials beneath the soils), and in urban areas, by 2) vehicle tire wear and industrial activity.
Disregarding the more local effects of road traffic and tire wear to look at only state level average soil concentrations of zinc, reveals a statistically-significant inverse or negative relationship between zinc levels in indoor and outdoor dust on COVID19 mortality in the USA. The trend is that the higher the average zinc concentrations in the soils of any given state, the lower is the average COVID19 death rate in that state. Note while examining the graph below that the soils of large parts of Washington state, Oregon, and Hawaii are underlain by especially zinc-rich basaltic rock:1
Food and drink both provide significant amounts of organic compounds, polyphenols, that – like prescription HCQ -- act as zinc ionophores. Quercetin, for example, is found in very high concentrations in elderberries, Mexican oregano, capers, cloves, and dark chocolate, and in moderately high concentrations in onions, bilberry, orange juice, red wine, apple, and other vegetables. 2 Epigallocatechin gallate is found in extremely high concentrations in green tea, and in moderately high concentrations in black tea, pecans, and hazelnuts.3 Although no laboratory confirmation has yet directly confirmed that they function as in vitro or in vivo zinc ionophores, the polyphenols (chalcones: xanthohumols) found especially in ales like dry-hopped IPAs and pale ales,4 as well as vegetables like broad beans (chalcones: butein), are known to form chemical complexes with zinc.
So, turning to the likely influence of background, regionally-variable dietary habits leading to ingestion of different levels of zinc ionophores and apparently consequent variations in US state to state COVID19 mortality rates, provides the following interesting series of scatter diagrams using USA state by state data. Note in each graph that, like was already seen for zinc metal, the trend is that the greater the general consumption of food or drink stuff known to contain significant quantities of polyphenols in a state, the lower is the COVID19 death rate in that state.
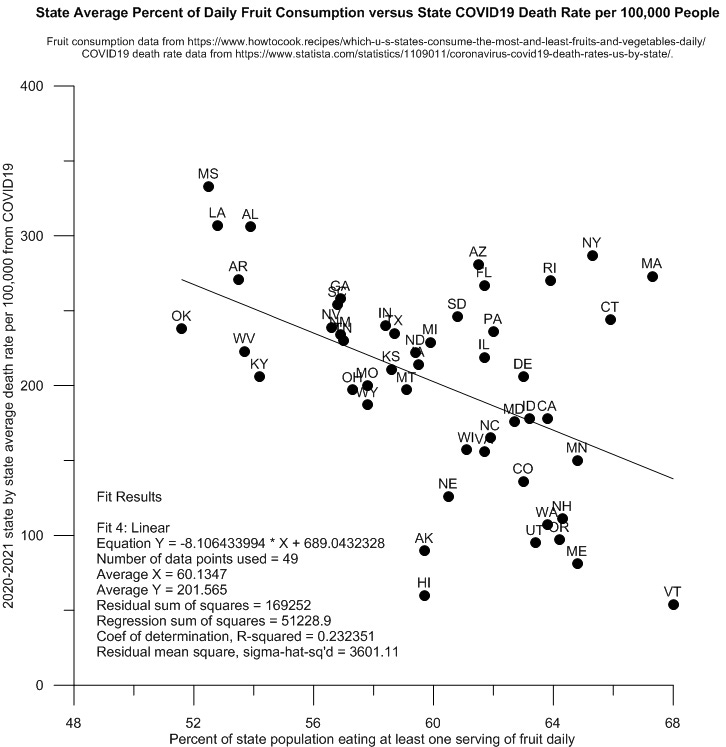
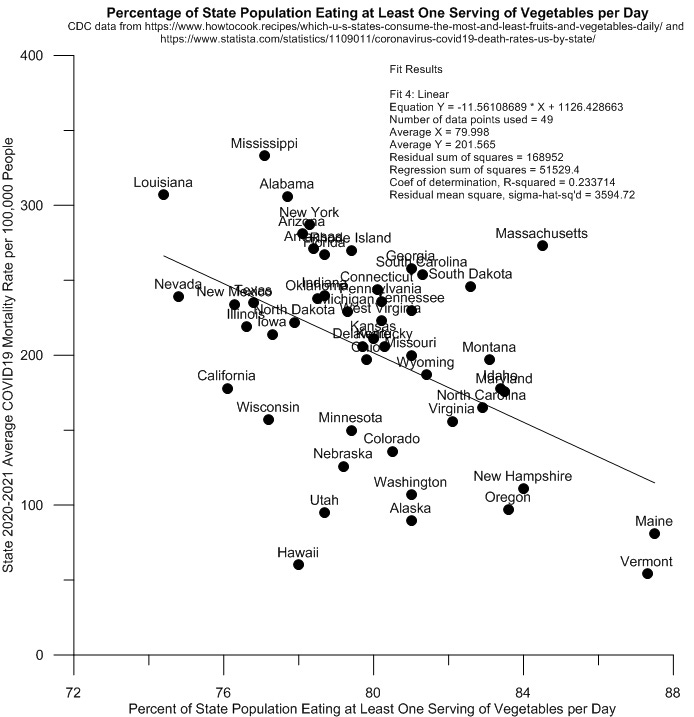
It appears that Vermont and Maine, with their higher than national average habits of eating polyphenol-rich fruits, vegetables, and higher than national average habit of drinking polyphenol-bearing craft beers, serendipitously prepared themselves very well for COVID19.
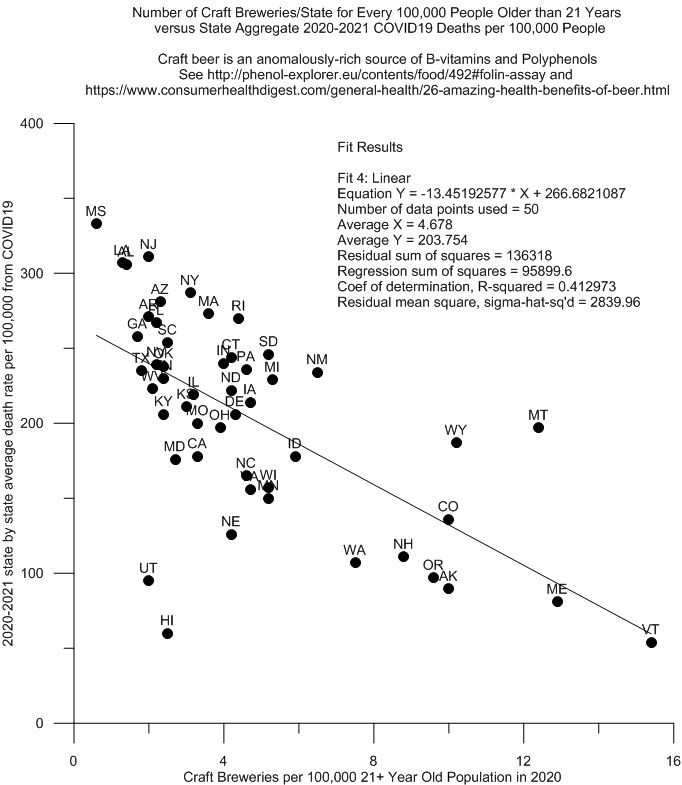
Of all the natural factors examined here, the strength of the relationship between the regional habit of drinking craft beer and experiencing low adult COVID19 death rates is the strongest. The r-squared value for this relationship (see graph above) suggests that as much as 41% of the variation in adult state-to-state COVID19 death rate can be explained by the relative availability of such beers and ales in the American states. As far as dietary intake of zinc ionophores is concerned, it appears that craft brews are, functionally speaking, the green teas of the US…
The same is true for part of northeastern Minnesota.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC4808895/ reports that green and black tea are also important sources of quercetin, a finding not reflected at the Phenol Explorer website at http://phenol-explorer.eu.
https://ift.onlinelibrary.wiley.com/doi/full/10.1111/1541-4337.12352 As will be discussed in a later post, unfiltered and unpasteurized beers and ales also contain high concentrations of B vitamins, including vitamin B3 (niacin) that likely explain craft beer drinkers’ apparent higher level immunity to COVID19 . These B-vitamins are derived from the brewers yeast used to ferment the sugars in the ale or beer worts. Beer and ale drinkers reportedly have an average of 30% more B-vitamins in their bodies than non-drinkers.
68 yo case study here FWIW. So far, no ro. Will not be jabbed. Have been taking NAC, niacin & VD3 regularly, added quercitin & zinc earlier this year. Fairly healthy, slightly overweight. Taking zero prescription drugs. Diet usually low carb, meat & veggies. Lived in CO last 15 yrs, now in SC. I don’t always drink beer, but when I do, it’s usually an IPA.
Great research, thanks!
It would be interesting to see what the impact of COVID19 is on those working in and around Zn rich mining operations. We know for a fact that Miners and Geologists are also known to tip a pint every so often! Should theoretically be a pretty healthy bunch😉!